














 38 / 156
38 / 156

36
IQ) as the BMR for IQ, a 1% increase in systolic blood pressure (SBP)
(equivalent to a 1.2 mmHg change) as the BMR for cardiovascular
effects; anda10% increase inexpected incidenceof chronic kidney
disease as the BMR for nephrotoxicity (EFSA 2010, Table 1).
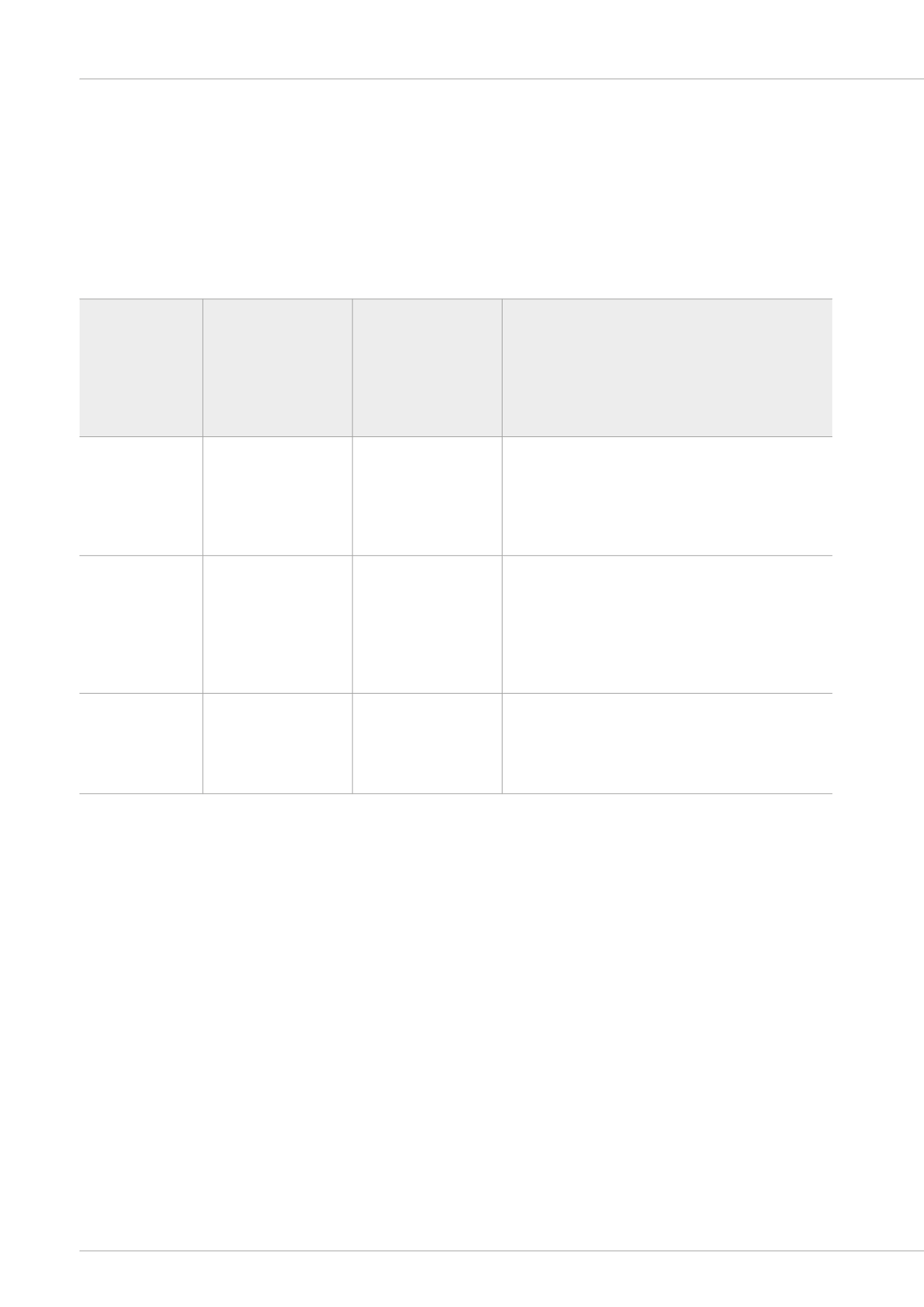
Table 1:
Critical effects of lead, associated blood lead levels and corresponding dietary lead intake values
identified by the EFSA Panel on
Contaminants in the Food Chain (CONTAM – EFSA 2010)
Benchmark
Response (BMR)
BMDL (95th percentile
lower confidence limit
of the benchmark dose
– BMD of extra risk)
derived from blood
lead levels (μg/L)
Corresponding dietary
lead intake value (μg/
kg bw per day)
Population level effects of BMR
A 1% (1 point)
reduction in IQ in
young children
BMDL
01
= 12
0.50
The BMR for IQ could impact the socioeconomic status of
a population and its productivity. Studies in the USA have
related a 1 point reduction in IQ to a 4.5% increased risk of
failure to graduate from high school and a 2% decrease in
productivity in later life (Schwartz 1994, Grosse
et al.
2002).
A 1% increase
in systolic blood
pressure (SBP) in
adults (equivalent
to a 1.2 mm Hg
change)
BMDL
01
= 36
1.50
A 1% increase in SBP has been related to an increase in
the percentage of the population treated for hypertension
by 3.1%, and a 2.6% or 2.4% increase in expected annual
mortality from cerebral stroke or myocardial infarction
respectively (Selmer
et al.
2000).
A 10% increase in
expected incidence
of chronic kidney
disease in adults
BMDL
10
= 15
0.63
The JECFA PTWI was subsequently withdrawn in 2010/2011
(WHO 2007, JECFA 2010, WHO 2011).
EFSA findings on the hazards to
human health from dietary lead
in Europe
The EFSA CONTAM Panel used the Integrated Exposure Uptake
Biokinetic (IEUBK 2010) Model for lead in children (IEUBKwin
version 1.1) and an equation from Carlisle and Wade (1992)
for lead in adults to estimate the dietary intake of lead
(BMD) required to produce the elevations in B-Pb associated
with the BMR and also the BMDL, the lower one-sided 95%
confidence bound of the BMDs (Table 1). This modification
of the BMD allows for uncertainty in the dose-response
relationship. They also assessed data on lead concentrations
in foods in the European Union, including lead directly derived
from ammunition in game meat. EFSA used information
on lead concentrations in food and amounts of food eaten
by individuals in participating countries to calculate mean
(‘average base diet’) and 95th percentile (‘high base diet’)
lead dietary exposures separately for each country. These
exposure data were then used to produce corresponding B-Pb
concentrations, and these were compared with the BMDLs
to evaluate risk. In some assessments, groups of people
frequently consuming game meat (defined as one 200 g meal
per week of game) were considered separately. In calculating
the effects upon B-Pb of game meat consumption the EFSA
CONTAM Panel assumed that the bioavailability of dietary lead
directly derived from ammunition was the same as for other
sources of dietary lead. They obtained the ratio of dietary
exposure, assuming various diets, to the BMDLs. The risk of
Rhys E. Green & Deborah J. Pain